Tendon and ligament injuries, and their subsequent repair and rehabilitation, have been prime concerns of equine veterinarians since horses began running, jumping and undergoing the stresses of competition.

© Amy K. Dragoo
The more recent addition of regenerative medicine products such as stem cells, platelet-rich plasma (PRP), Interlukin-1 receptor antagonist protein (IRAP) and others have provided the clinician with a means of improving and accelerating the repair process. These products provide a scaffolding for the early realignment of fibers within an injury and help improve the local tendon or ligament cellular environment to speed healing.
However, the challenge has been to find accurate ways to initially diagnose the scope and extent of tendon and ligament damage, to stage the timing of reparative injections and treatment, and to be able to quantify [measure] and monitor repair and healing.
Limitations of Conventional Ultrasound
Ultrasound has long been the standard modality for diagnosis of soft tissue (muscle, tendon and ligament) injuries. It allows the veterinarian to “see” fiber patterns and to diagnose situations. These situations include:
- major tears with well-defined fluid filled “holes.” When tendons and ligaments suffer significant tearing and fiber separation, cellular fluid released from the trauma fills in the space creating a dark “hole” on ultrasound. Fluid appears black on ultrasound.
- areas with scattered, shredded tendon fibers and fluid or edema through a length of the structure. In these types of injuries, the damage is variable, so there may be thin, fluid-filled or dark areas in an irregular pattern throughout the area of concern.
- minor areas of pattern disruption or simple thickening. There is no tendon damage that causes edema or fluid production, so no dark areas—just thicker, wider structures with less well-defined fiber patterns.
Courtesy, Hans T.M. van Schie, DVM, PhD
Unfortunately, ultrasound has its drawbacks, as well. For example, it is a static modality that provides only a single specific view of an area in one moment in time. Therefore, it does not provide active physiologically useful information. For instance, ultrasound scans of a cadaver limb are indistinguishable from those of a live horse. Additionally, often ultrasound cannot show early changes or differentiate stages of healing.
The physiologic processes of both injury and repair are subtle and constantly changing. As a result, ultrasound does not always provide an accurate representation. Conventional ultrasound is not generally considered sensitive enough to monitor tendon repair. Certainly it is not capable of predicting injury. Tendons can be functionally more damaged than they sometimes appear on ultrasound. Or there may be substantially more healing of a lesion than appears on the screen.
Courtesy, Hans T.M. van Schie, DVM, PhD
Courtesy, Hans T.M. van Schie, DVM, PhD
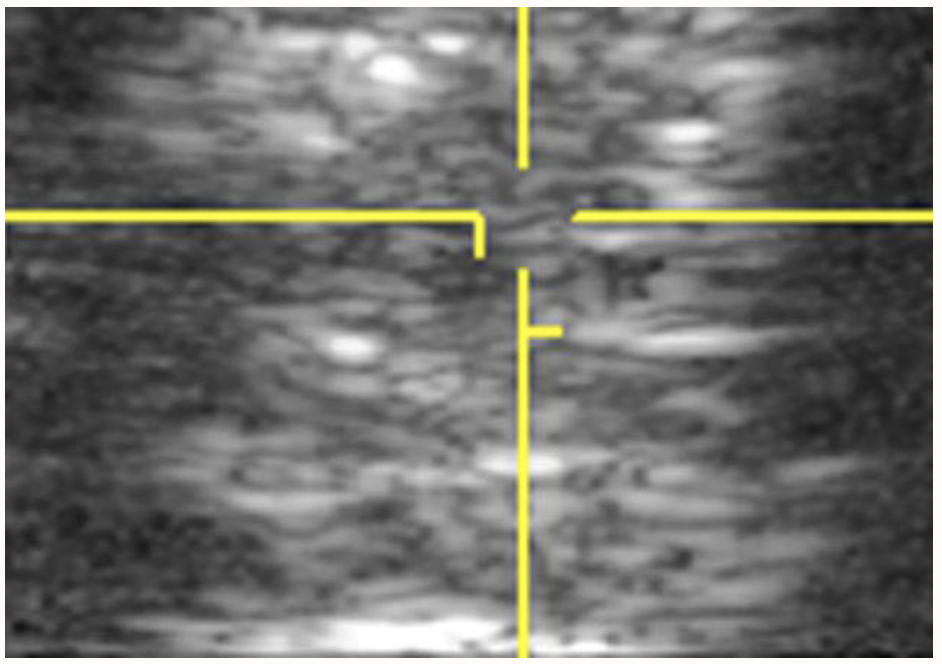
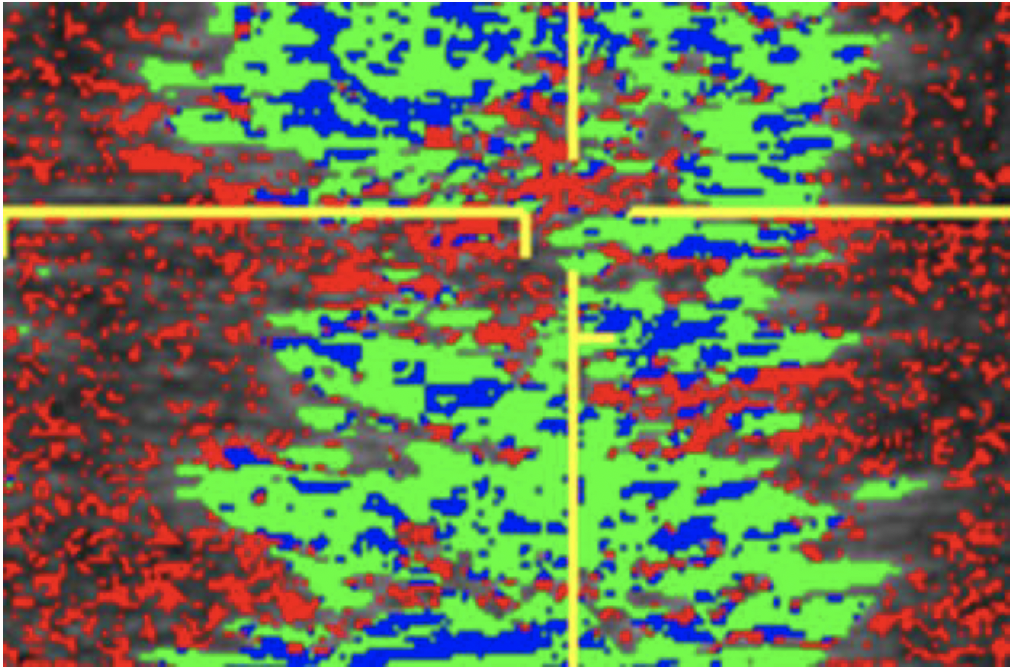
Ultrasound Tissue Characterization
Recently, in both human and veterinary medicine, the technique of ultrasound tissue characterization, also known as UTC, has been utilized to fill in the gaps created by traditional ultrasound. In this technique, a standard ultrasound probe is placed in a motorized tracking device. This device is placed on the horse’s skin over the tendons. The probe is automatically moved along a track that allows it to uniformly scan a length of leg. A 12-centimeter length is scanned in 45 seconds. Images are captured every 0.2 millimeters. The over 600 images and information produced are digitally manipulated to generate a 3D tendon representation.
This precise “spatial stacking” of images provides a much more detailed and accurate representation of the tendon and various areas along the scanned length. This is proving extremely helpful, as most tendon injuries are found to involve varying lengths and depths along the limb with pockets of better fibers intermixed with areas of more serious damage. This subtlety is missed with a standard ultrasound but is better defined with 3D tissue characterization.
The ability to, in a standardized and repeatable way, rescan the exact same area and create another 3D representation in two weeks or so allows the clinician to monitor specific areas within the tendon and to stay focused on those individual areas and the repair process. This more directed monitoring opens the door to more correct utilization of other treatment options such as specific injections of regenerative products into certain nonhealing or slowly responding areas, even when closely surrounding tissue is healing well. It will allow the use of shockwave therapy, pulsed electromagnetic wave therapy or other modalities in other directed areas when necessary and better incorporation of physical therapy at appropriate times.
More specific information allows for more specific treatment, and that generates better overall results. Most of the therapies for tendon and ligament treatment have been available for some time, and there are no dramatic recent developments. However, with ultrasound tissue characterization techniques, the ability to more specifically and accurately utilize these treatments will likely translate into greatly improved tendon repair.
It is also hoped that ultrasound tissue characterization will help predict tendon and ligament injury. Routine sequential scanning and comparison of horses in training might be able to characterize early tissue thickening or fiber-pattern disruption as an early indicator of impending damage. This aspect has not yet been fully investigated, but the research and veterinary community remain hopeful.
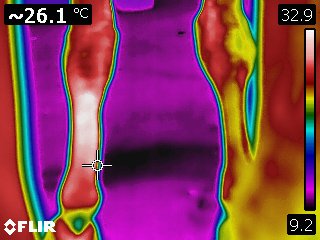
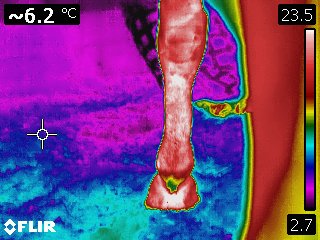
Revisiting Infrared Thermography
One often overlooked diagnostic modality that has already proven to be very beneficial in diagnosing tendon and ligament injuries is infrared thermography. This modality is capable of accurately providing information on the dynamic healing of these structures, as well as predicting injury. Dr. Tracy Turner, DVM, published landmark research detailing that infrared thermography showed a high degree of clinical correlation with tendon and ligament injuries in Thoroughbred racehorses in training. It also noted that thermography could locate and detect impending tendon damage an average of two weeks before changes were noted on ultrasound.
This research led many racehorse stables to incorporate thermographic scans of all horses in training. They used the resultant data to alter training intensity to reduce injury and wastage. Thermography has also been used successfully for tendon and ligament injury diagnosis and the treatment and staging of rehabilitation in multiple disciplines. English disciplines include jumping, dressage and eventing, and Western includes reining and cutting.
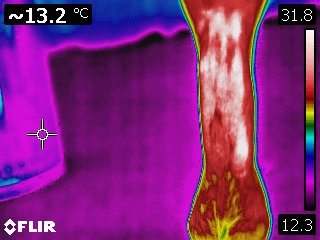
Infrared thermography is a dynamic modality providing a detailed, real-time image of the physiology of an area. It also provides an evaluation of the intensity and distribution of the heat associated with a tendon or ligament. As such, it is a method for specifically and repeatedly monitoring the extent of initial damage and to follow the repair process. Because thermography can accurately and repeatedly differentiate between various areas of tendon within a larger damaged area, sequential scans can provide useful information for treatment and in the repair process, as well.
Courtesy Kenneth Marcella, DVM
Courtesy Kenneth Marcella, DVM
Courtesy Kenneth Marcella, DVM
Although it was the most-requested diagnostic modality at the 1996 Olympics in Atlanta and has been extensively researched and used in both human and veterinary diagnostics, infrared thermography remains less well known than ultrasound. In addition, there is a steep learning curve associated with its correct use and application. But this modality has many distinct advantages over traditional ultrasound.
Ultimately, the combined use of ultrasound tissue characterization and sequential thermography scans might prove to be the most accurate combination of modalities to diagnose, manage repair and direct successful rehabilitation of tendon and ligament injury. This use may also lead to advances in the early prediction—and therefore avoidance—of injuries.
The Best Option: Wowie’s Story
Sometimes tried-and-true therapies are the most practical when treating tendon injuries.
All too often, a horse comes up from the pasture with an injured tendon—and the guesswork begins: How did this happen? What exactly is damaged? What are the best ways to treat this injury, given this particular horse and his owner’s goals, not to mention budget?

Courtesy, Stacey Wigmore
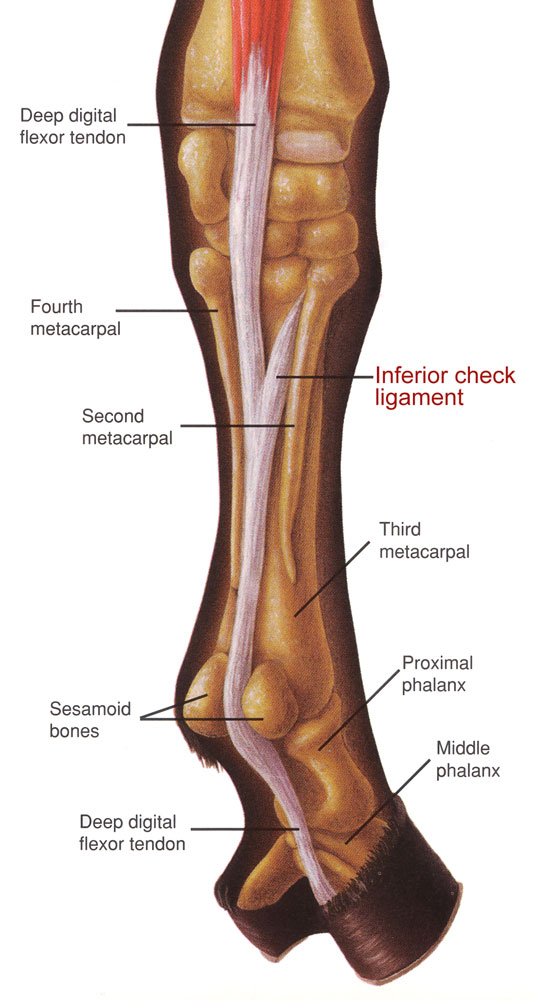
Such was the case in 2011 when an 8-year-old, off-the-track Thoroughbred named Wowie emerged from the field with a “significant” swelling low on his right-hind leg. “Best guess is that he injured himself running around his very hilly (and sometimes slippery) pasture,” recalled his owner, Maryland resident Stacey Wigmore. “The swelling was hot, and he was unsound. I sent photos to the vet. He was concerned and came out and used ultrasound to diagnose a deep digital flexor tendon tear that was 2 centimeters in size.”
The prognosis for this type of injury, which is somewhat unusual in a hind limb, wasn’t very promising. Wigmore and her veterinarian discussed treatment options but ruled out the use of PRP (platelet-rich plasma) and IRAP (interleukin-1 receptor antagonist protein), the newest high-tech treatments at that time, in favor of more conventional treatment. “We agreed that dropping that kind of money on a $500 horse wasn’t practical, despite Wowie being a wonderful, level-headed partner with a little talent,” Wigmore explained. “I was not offended by this,” she added, noting, “I very much appreciated that just because we could didn’t mean it was the best treatment option in this case.”
Atypical Rehab
Because of Wowie’s boarding situation at the time, his rehab protocol wasn’t exactly typical.
“In a perfect world, Wowie would have been on stall rest for 30 days,” Wigmore explained. “But all the horses at the farm lived outside, and he demonstrated that he was going to hurt himself more if I tried to keep him in a stall, even with his buddy next to him.”
So Wowie’s somewhat unconventional-yet-conventional treatment got underway with non-steroidal anti-inflammatory drugs, cold-hosing, daily alternating of poultices and sweats, and standing wraps on both back legs. His concerned owner checked on him once or twice every day.
“I started by keeping him in a smaller paddock with his friend at night, and he went out in the larger, flat field during the day as long as he stayed calm,” Wigmore related.
Shockwave Treatments
In addition, Wigmore’s vet elected to perform two shockwave therapy treatments a couple of weeks apart. “I recall the first one was quite soon after the diagnosis (maybe a week or two). The second was a couple weeks to a month after that,” she said.
Extracorporeal shockwave therapy is a noninvasive procedure that has reportedly been used in horses since the 1990s. It directs high-intensity acoustic energy pulses toward a specific region of the body, reducing inflammation while increasing circulation. This, of course, helps stimulate healing in wounds and musculoskeletal or soft-tissue injuries. Shockwave therapy is also said to help release muscle tension, accelerate bone growth and provide temporary pain relief.
Nowadays, shockwave therapy is used for maintenance applications, too, such as slowing the progression of arthritis and addressing pathologies like “kissing spines.”
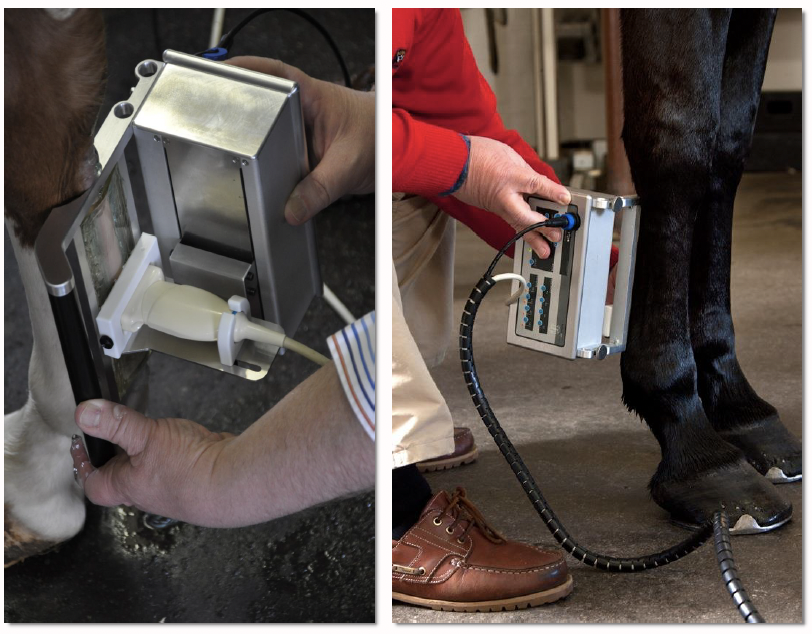
As Wigmore recalled, the whole process took only a few minutes. It involved a small portable machine, some light sedation for Wowie, and the use of a wand, or probe, guided by hand over the affected area.
Full Recovery
An ultrasound reading about two and a half months later confirmed that Wowie’s tendon was healing well, with the fibers lining up as hoped. Because the gelding was also trotting soundly at that point, it was deemed appropriate to start slow work under-saddle, gradually increasing the times, distances and speeds.
Five or six months after his injury, Wowie was cleared by his vet to go back to full work, which Wigmore continued to take slowly. “He was soon back in the show ring, doing 2-foot to 2-foot-3 hunters for the rest of the season,” she said. “He went on to have a full career with no limitations, training and competing at local and Thoroughbred shows up to 3-foot hunters and jumpers for around a decade.”

Courtesy, Stacey Wigmore
The lesson to this story: Though cutting-edge procedures are available for tendon injuries, never underestimate the ability of more established technologies and good, old-fashioned rehab to get the job done.
“I did the best I could with what I had available at the time, and somehow I got lucky,” Wigmore commented. “While high tech-therapies are wonderful tools, I truly believe that they’re not always the best options. And owners shouldn’t feel guilty about trying more conservative treatments first.”
But, as she cautioned, “Every horse and situation is different. I’d definitely recommend coming up with and following a rehab protocol in collaboration with a trusted vet.”
—Sidebar authored by Laurel Scott
About Kenneth L. Marcella, DVM
Kenneth L. Marcella, DVM, is a graduate of the New York State College of Veterinary Medicine at Cornell University. For more than 30 years, he has treated sporthorses of all disciplines and levels, including international competitors.
Dr. Marcella has served as a veterinary official at many events around the world, including national championships, World Championships and Olympic competitions. He is board-certified in thermal imaging and is currently a member of the board of directors of the American Academy of Thermology. With an undergraduate degree in English from Dartmouth College, Dr. Marcella has also written articles for numerous publications, including Dressage Today, DVM 360, Endurance News, The American Quarter Horse Journal and Thoroughbred Times. In his free time, he plays and coaches hockey.